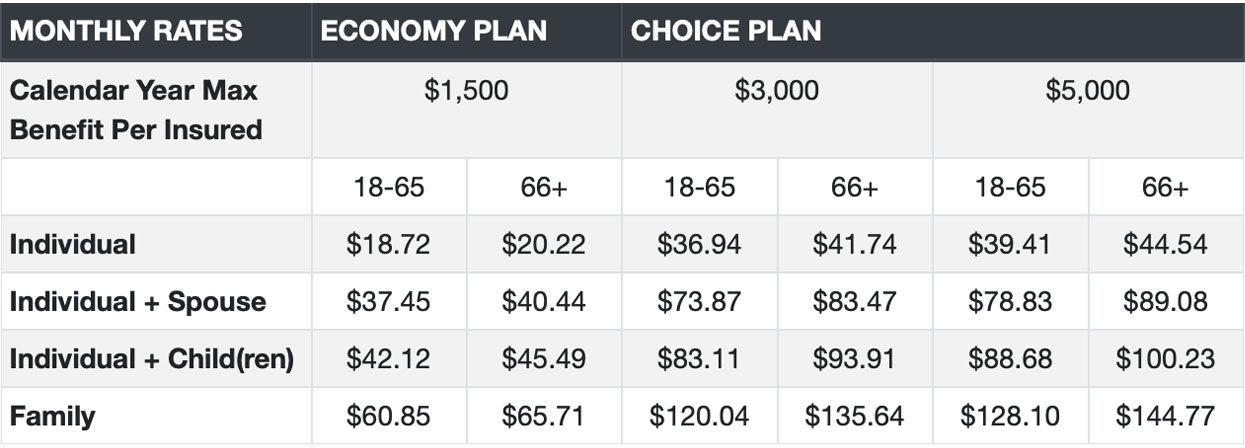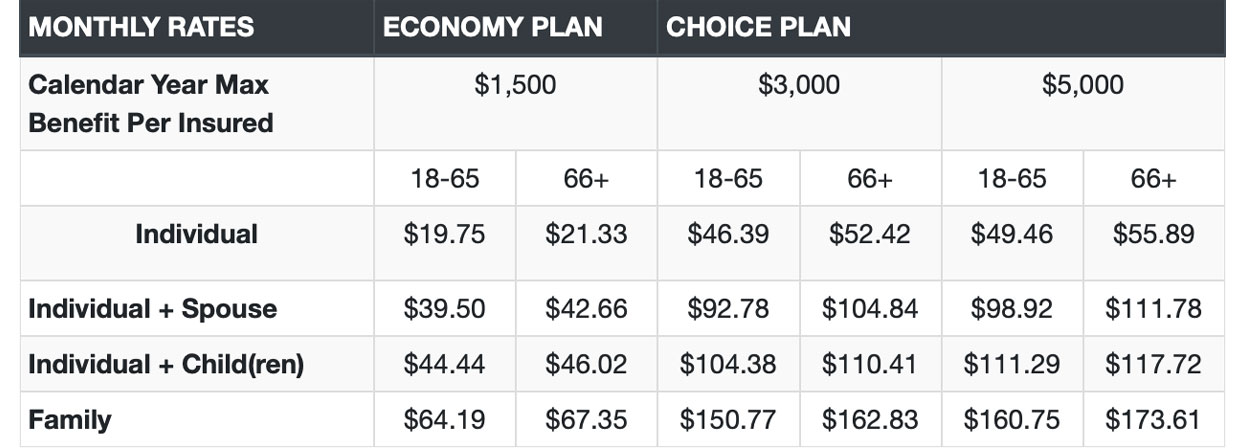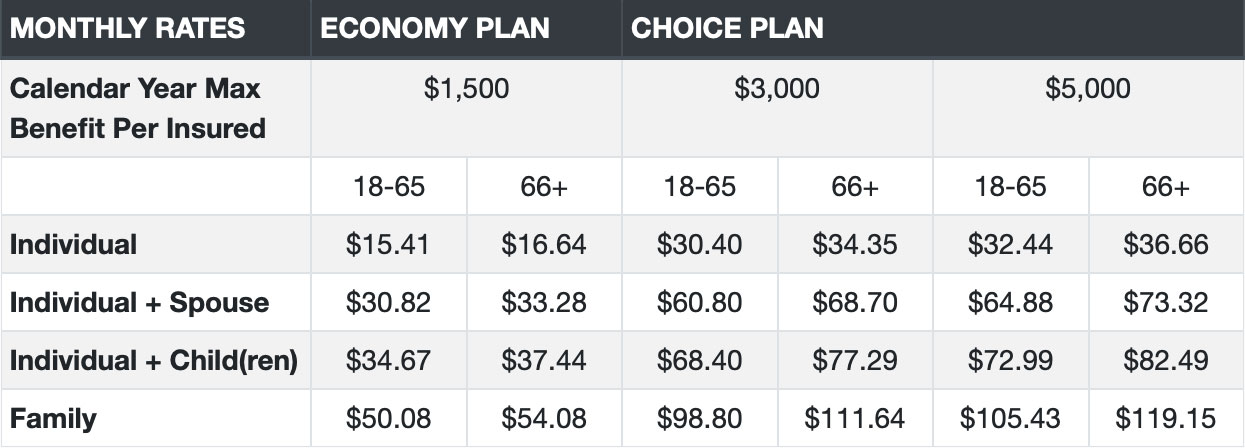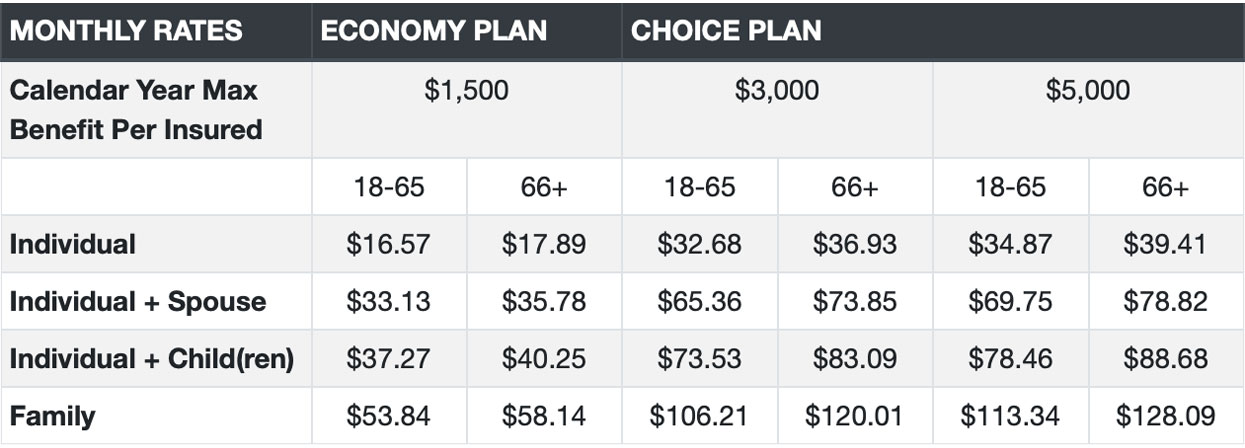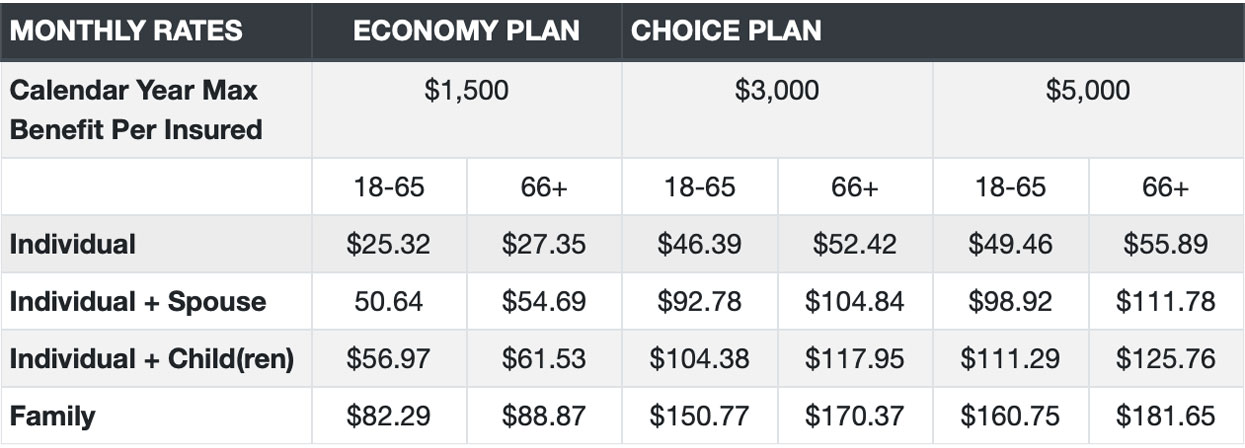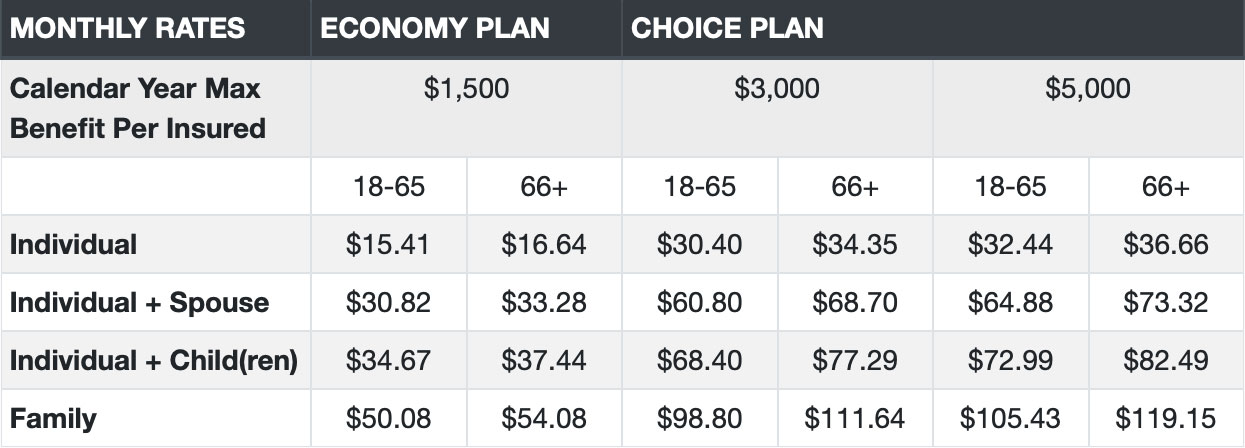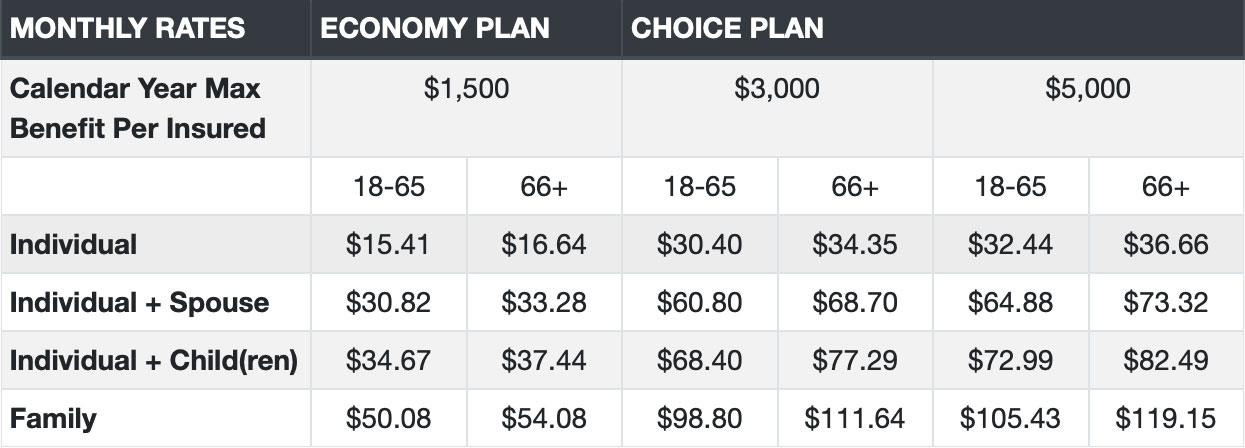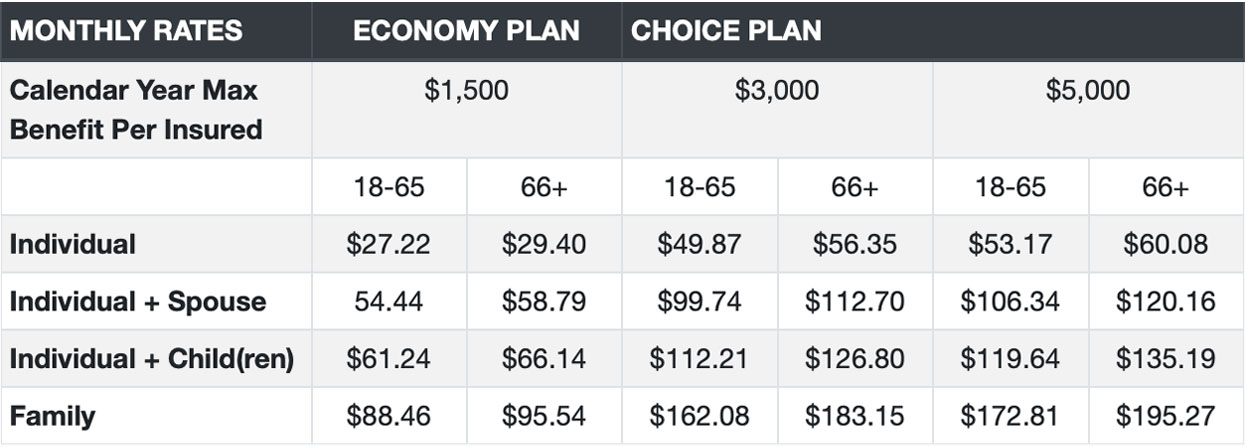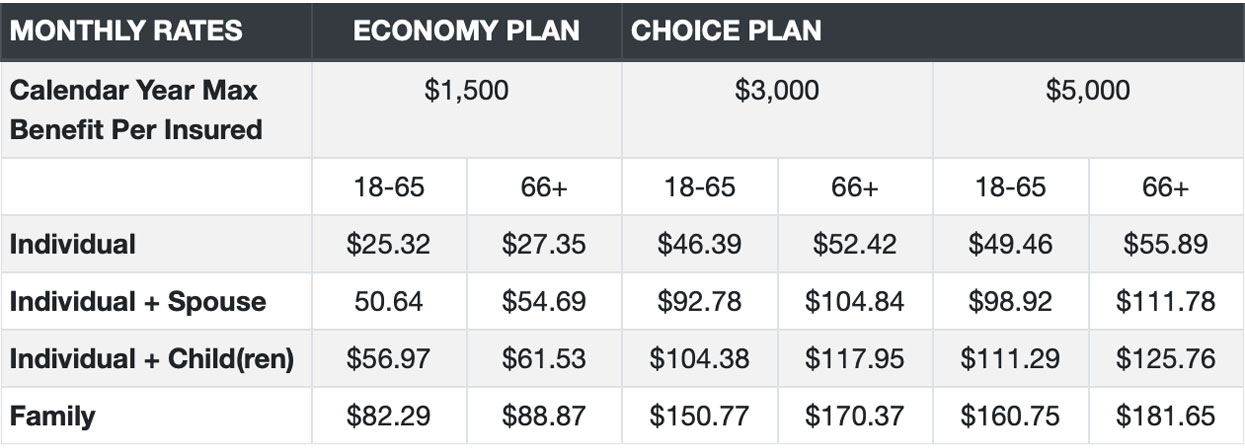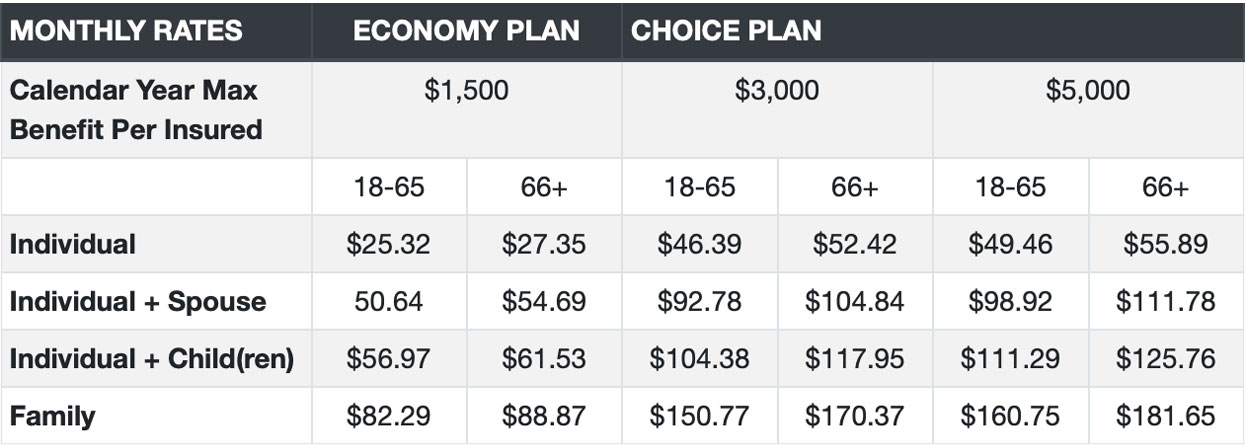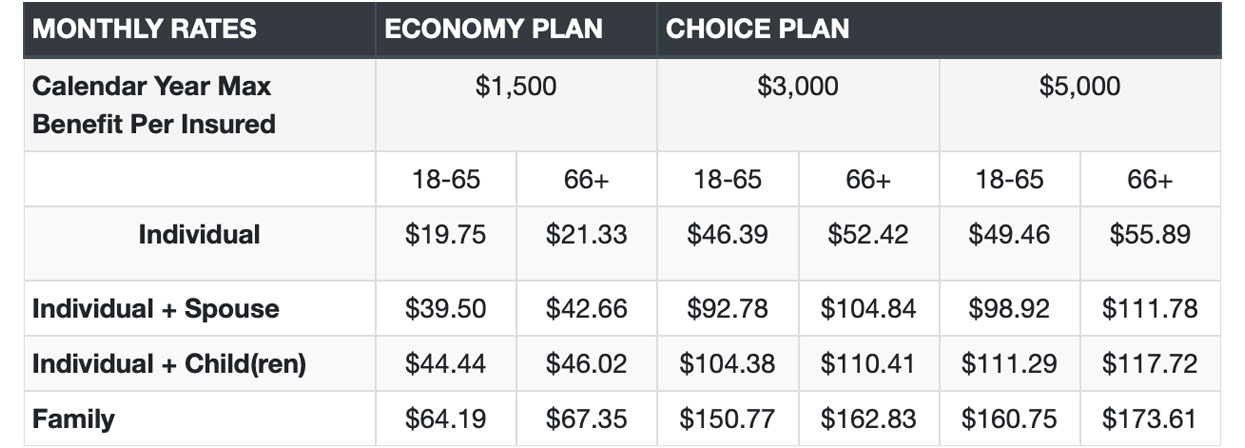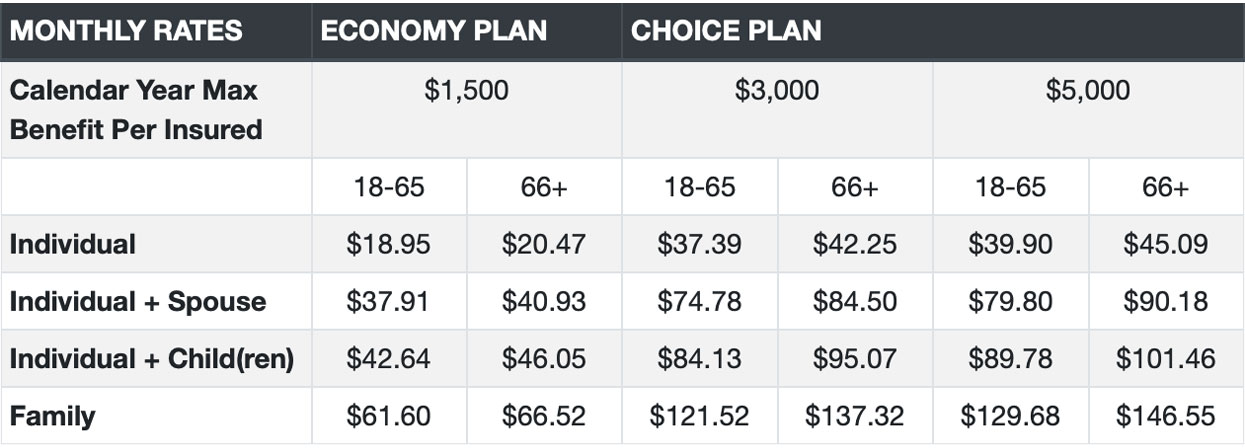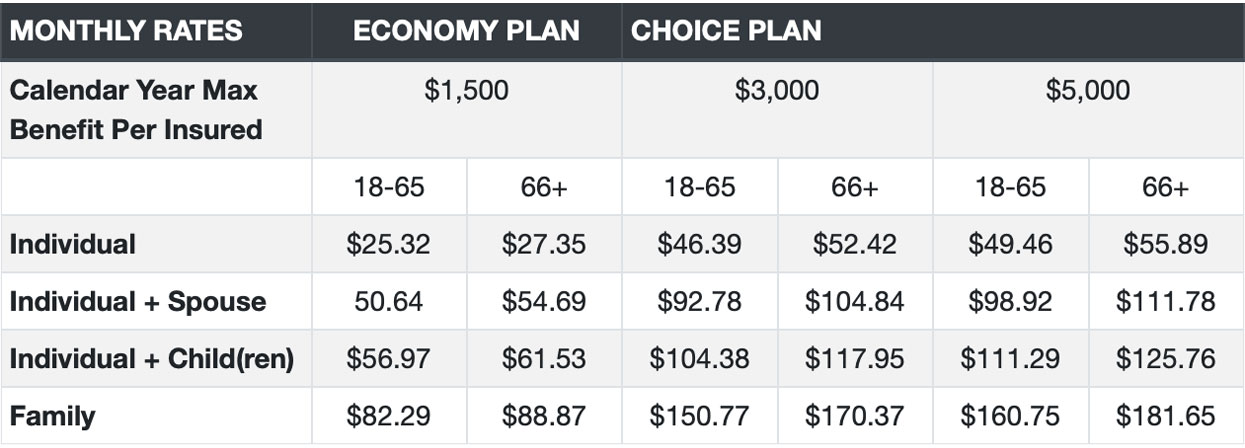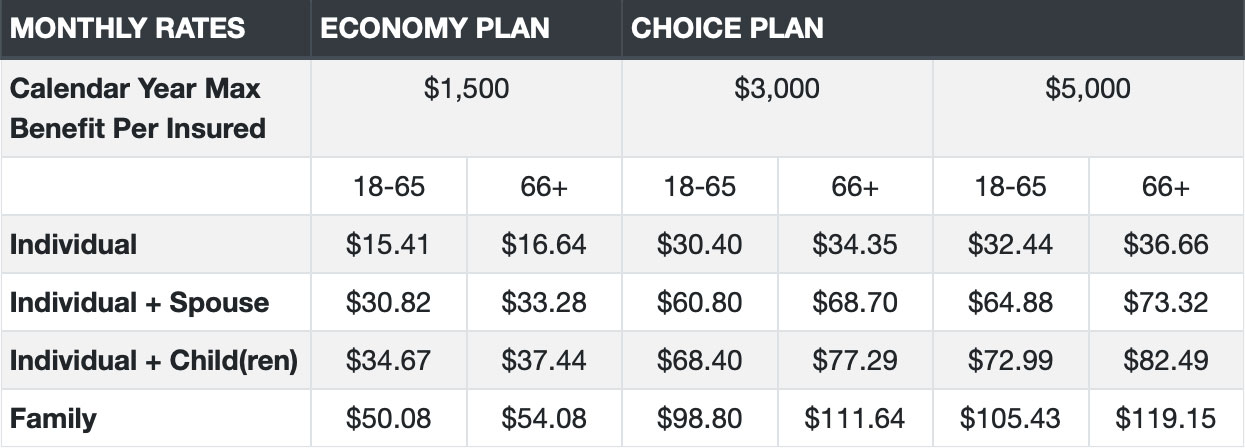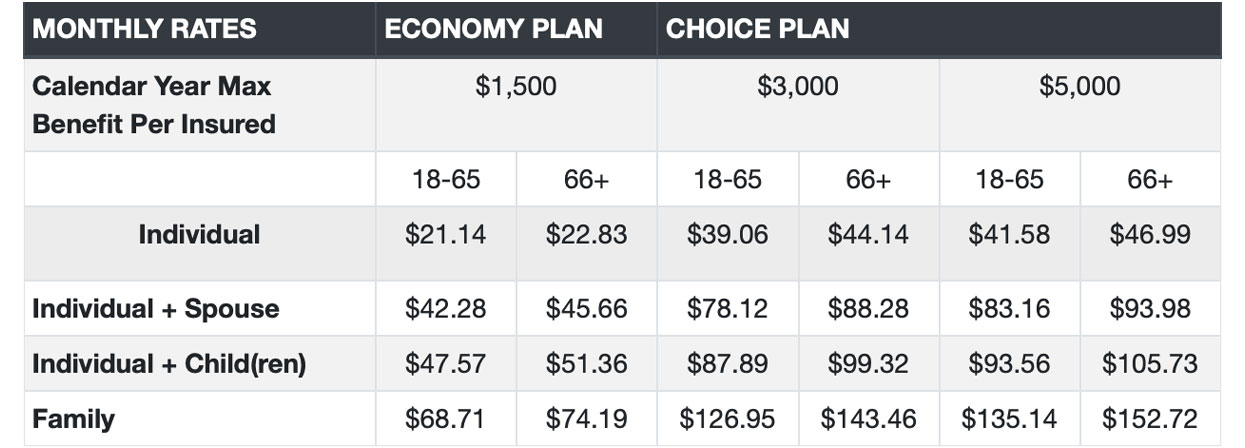




There is No waiting period on the Choice Plan $3000 and $5000 annual maximum options. There is No waiting period on the Economy Plan $1500 annual maximum option for Basic Services but there is a 6 month waiting period for Intermediate Services.
Yes. Our National Networks of Dentemax and Connection Dental have over 20 million members and over 265,000 Provider Access Points.
Yes – Each covered child has the same annual maximum and benefits as the covered adults.
Yes. Please see brochure for details.
There are No Deductibles, only a $25 co-pay per visit. Coinsurance applies on certain procedures.
No claim forms required when using in-network dentists. If you were to go out of network then claim forms would be required.
You will have a choice during the online enrollment to select the 1st or the 15th of the month for an effective date. If you select a 1st of the month effective date your initial billing will be the premium rate that was shown on the quote page. If you select a 15th of the month effective date your initial billing will be 1 ½ months premium to cover the first 45 days of your coverage. The initial billing will be processed upon submission of your application.

Best Dental Plan has a great affordable dental option and viewing rates by state is simple, with an easy quote and apply process.
Looking for dental coverage for my family was an ease, no waiting periods and no deductibles on the Choice Plan gave us the flexibility to get our family the coverage we need.
Choosing a dental plan can be exhausting, so many options, it's good to know they offer such great coverage, which helped me get my dental work done.